

This will be long, so please bear with me. The topic of veterinary bills and what goes into pricing is one that really needs to be discussed with every pet owner, but veterinary professionals rarely get the opportunity as it’s a sensitive subject on both sides…and can be complicated.
*cue foreboding music*
Before I get into the nitty gritty, please take a look at this excellent cost comparison:

An article by Dr. Doug Mader, DVM, MS.
Dr. Doug Mader is one of the most renowned doctors in veterinary medicine. He has been a past President of the North American Veterinary Conference, consults for several well-known zoos/aquariums and research/conservation programs, and is on the review/advisory boards for several highly respected scientific journals. Dr. Mader has written or contributed to almost every textbook used in modern veterinary and veterinary technology schools — not to mention his contributions fill the reference texts of almost every doctor’s office, especially those who happen to deal with reptiles. He speaks at numerous veterinary conferences across the country every year and is triple board certified (Canine/Feline, Reptile/Amphibian, and Herpetology). All of his immense education and expertise contributes to the reason surgery at his practice runs on the higher end of costs vs. a general practitioner.
The other reason his services run on the higher end is that he practices in a busy metro area that has a high cost of living with higher property taxes, mortgage rates, utility costs, and insurance premiums. It seems overwhelming, but all of those things play a role in veterinary pricing. Nonetheless, even with the incredible level of education and expertise behind it, his pricing can never compare to human medicine. $1600 vs. $16,000 is an immense difference!
Here is another fantastic example:
My husband recently went to the ER after suffering from a sudden onset of debilitating back pain that literally dropped him to his knees. He was examined by a doctor, had a set of thoracic radiographs taken, and was given an intramuscular corticosteroid injection then told to follow up with his regular physician. If he were to provide these same exact 3 services for one of our veterinary patients, their owner would pay precisely $203 plus tax. $32 for the office visit/exam, $150 for the radiographs, and $21 for the Depo-Medrol injection. When we received the statement from our health insurance company yesterday (to whom we pay a $2,000 premium per month for the 4 of us in our family), it was unsurprising that the total bill for that ER visit came out to $2,140 and some change — $1,632 of which we are responsible for out of pocket as part of our deductible.
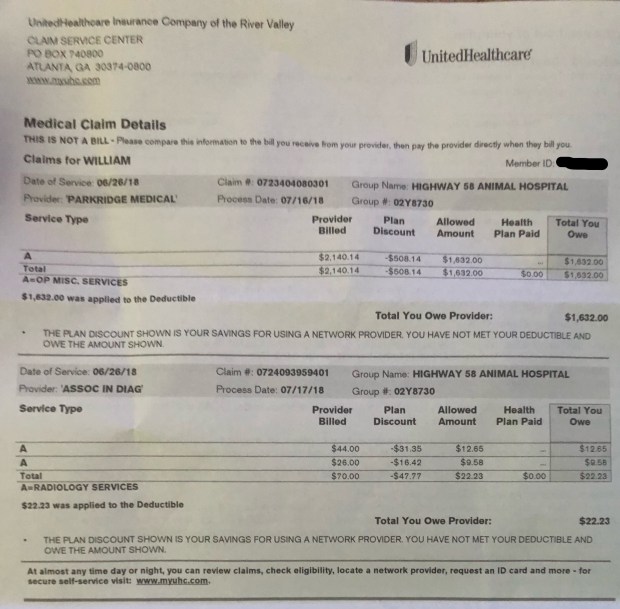
Our health insurance statement for the most recent ER visit.
What is the main issue?
At the base level, we frequently get accused of being “money hungry” or being “only in it for the money, not the animals”, which is far from the case for the vast majority of veterinary professionals. To be fair, some associate veterinarians have performance bonuses in their contracts, but this is minimal and not always a common practice. That “performance” is usually made of up of prevention products and preventive medicine, and is used as a way of encouraging doctors to encourage owners to take better care of their animals by testing for Heartworm, getting on Heartworm prevention, having dentals done, etc. Practice owners do not generally benefit from increased quarterly profit numbers, as most take an unchanging salary and anything else goes right back into the practice to be put toward improvements in equipment or supplies, building maintenance, etc.

The pin I earned upon graduation.
What is behind the title of LVT or DVM?
Your average licensed veterinary technician (CVT/RVT/LVT) has the same college degree, license, and yearly continuing education requirements as a human LPN/RN. We have associates, bachelors, and masters degrees, passed a national exam, maintain a state-regulated license to practice, and have to complete 12-15 hours of approved continuing education each year to maintain that license. We make $11-$16 per hour, with the most common range being $12-$14. Our student loans average $45,000-$90,000, depending on whether we attended public or private schools, whether we earned a 2-year or 4-year degree, etc.
Your average licensed veterinarian (DVM) has the same college degree, license, and yearly continuing education requirements as a human MD. A 4-year undergraduate degree in Animal Science, Biology, or similar, then a minimum of a 4-year veterinary doctorate (board-certified DVM’s go an additional 4-6 years). A DVM also has to pass a national exam, maintain a state-regulated license to practice, and has to complete 28-32 hours of RACE-approved continuing education each year to maintain that license. The average starting yearly salary for a general practice DVM is around $60,000 — a practice owner may make $70-$90k per year. Board-certified, emergency, and specialty practitioners make a bit more considering their education and specialty training/skills. Average student loans run $250,000 to $350,000. Veterinary school is one of the most expensive degree programs out there.
Both an LVT and a DVM have to know the anatomy, physiology, behavior, diseases, parasitology, hematology, endocrinology, cardiology, microbiology, nutrition, anesthesia, husbandry, pharmacology, reproduction, neonatal care, surgical procedures, normal vs. abnormal cell counts, vitals, chemistry panels, blood panels, etc. of multiple species AND multiple breeds within those species…instead of just humans. That doesn’t include the knowledge we also have to have on the operation and maintenance of various surgical instruments, diagnostic machines, a wide array of pharmaceuticals, radiology, imaging software, records software, medical terminology, and so much more.
What exactly do we do?
We work long 10-16 hour shifts on our feet, every single day including Saturdays, dealing all day long with patients who cannot speak or comprehend our language, don’t understand what we’re doing to them or that we’re trying to help them (and not hurt them), howl, growl, hiss, bark, scream, thrash, scratch, kick, bite, and leave giant scars all over our bodies…and then we tell you how “good” they were because we don’t want you to worry or feel bad. We express anal glands, trim nails, draw blood, examine poop samples, clean yeast-filled ears, scrape calculus off of and extract rotten teeth, pull out/off parasites, perform biopsies/surgeries, fix bones, remove cancer, remove dead necrotic tissue, lance boils and abscesses, and do just about every disgusting thing you can imagine. We go home covered in every bodily substance that exists, pick fleas and ticks off our scrubs and our hair, and end up with ringworm on our skin.
We deal with angry clients who don’t think they should have to pay $800 for having their sewing thread surgically removed from their cat’s intestines, or think $50 for 6 months of Heartworm prevention is “unnecessary” when they can “just use garlic and diatomaceous earth” (despite the fact that garlic is toxic and causes severe anemia). These clients swear at us, throw things, and degrade us for “not being real doctors/nurses”.
We are often the ones left holding animals when they take their last breath and slip away, whether it’s because we couldn’t fix what was wrong and they are dying on the treatment/operating table, or the owner couldn’t afford the necessary surgery/treatment, or the owner chose euthanasia and didn’t want to stick around. We stay professional, strong and supportive for our clients in their most painful moments…then go sit in our cars at the end of the day and cry our eyes out because someone just dumped their 10-year-old dog off to be euthanized after they got a new puppy and the dog didn’t get along with it; or because we tried everything under the sun, even things we didn’t charge the client for that they don’t even know about, yet couldn’t save a tiny 6-week-old kitten, and then we have to go tell a little girl that her new kitten didn’t make it…all the while thinking of our own daughter and how the kitten looked exactly like the one we have at home.
The veterinary profession has a suicide rate that is 2-4 times that of the general population, making it one of the highest in the world. This statistic isn’t just in the U.S. either — it spans the profession across the UK, Europe, and Australia as well.
New Study Finds Higher Than Expected Number of Suicide Deaths Among U.S. Veterinarians
Veterinarians Face Disproportionately High Suicide Rates, Study Says
Suicides among veterinarians become a growing problem
Suicide trend in the profession stretches back decades
The reason is usually emotional and psychological burn-out after repeatedly enduring the things I just described above. If that isn’t difficult enough, then we have to handle clients who are upset about prices or payments, constantly fight against Dr. Google and all the horrible advice on the internet, and people constantly trashing us on social media or sharing their personal anecdotes that apparently somehow outweigh years of education and expertise.
One of the most well-known losses to our community has been Dr. Sophia Yin, who was a world-renowned animal behaviorist and dog training expert, and one of the driving forces behind the positive-reinforcement training method. Dr. Yin authored numerous magazine articles, books, and veterinary textbooks, and produced many educational and instructional DVDs (which we used in our behavior semester while I was in college). Dr. Yin served on the executive board of the American Veterinary Society of Animal Behavior, and was on the American Association of Feline Practitioners (AAFP) Handling Guidelines Committee as well as the American Humane Association’s Animal Behavior and Training Advisory Committee. She lectured around the world to veterinarians and animal professionals, teaching seminars and workshops on animal behavior and low stress handling for dogs and cats. Yin also consulted for zoos and shelters, as well as several popular shows on Animal Planet.
Sophia Yin committed suicide on September 28th, 2014 at the age of 48.

Dr. Sophia Yin, DVM, MS
What makes our profession different from human medicine?
Many clients and the general public often compare their expectations of us to those of our human counterparts. However, we have vast differences — aside from the species we treat, of course.
Unlike human hospitals, we don’t have billion-dollar trust funds filled by donations or investors, and our patient bills don’t get paid by insurance companies. Pet insurance does exist, but it does not bill directly the same way human health insurance does. It requires payment up front by the client, then they wait to be reimbursed. Unfortunately most pet owners do not utilize it yet.
Also unlike human hospitals with huge bankrolls, every single dollar the clinic makes goes RIGHT back into payroll for doctors, techs, kennel staff, receptionists, janitors, etc. as well as equipment rentals/repairs/maintenance/upgrades, dry goods such as food and supplements, medications/syringes/needles/gauze/other medical supplies, electric bills, water bills, trash/biohazard disposal, software licensing and server backup, property taxes, mortgage payments, malpractice insurance, liability insurance, you name it. Our property taxes this year were approximately $20,000 out of pocket. A practice in Miami or Chicago will pay far more than that.
It is a very delicate balance to maintain a veterinary practice. I won’t even touch the topic of staff payroll, as we are chronically underpaid for our level of education and abilities. Many licensed technicians (with degrees) leave veterinary medicine altogether after a few years, as they cannot afford to support their families on $12/hour.
Then we have the equipment needed to properly diagnose and treat our patients. Do you know how much that digital x-ray machine along with the licensed software costs a clinic out of pocket? How about the ultrasonic dental scaler? The anesthesia equipment? The blood diagnostic machines? The ultrasound machine, or those overhead surgery lights, or that $2500 fluid pump keeping that cat with kidney failure alive? We have 6 of those. Most hospitals have over a dozen or more.
All the equipment we use has to be purchased or leased, maintained, updated, fixed, and backed up (software). Charging $150 for a set of radiographs (x-rays) barely chips into the $25,000 up front cost we paid to buy it so that we could provide better, clearer diagnostic imagery; for example, all of the Labradors and German Shepherds we see with hip issues.
Advances in diagnostics are leading to the demand for CT imaging, which greatly increases the ability to find sub-gingival dental problems, bone fractures, and malignant tumors that otherwise love to hide — among other things. We just paid $180,000 for our CT machine and accompanying software which takes the scan and renders a 3D image that can be manipulated and examined in depth. This was a bargain — yet some clients still scoff at the $250 charge (which includes anesthesia, IV contrast dye, etc.) despite the fact that there is NO hospital within a 1,000 mile radius offering CT imaging at that price, and we are one of less than a dozen general practices across the country that even offer CT imaging. Most CT machines are at specialty hospitals or emergency practices, and a scan typically runs $800-$2,000. Yet in spite of the scoffs and balking at the price, however low ours may be, this new diagnostic tool has already helped us discover countless tumors that we otherwise never could have seen, and save dozens — if not going into hundreds — of patients’ lives. Our own cat was one of the patients for whom CT was a priceless diagnostic opportunity.

Billion, my beloved Himalayan mix who passed from metastatic lung cancer at age 7.
Why can’t we be more flexible or help more clients who are struggling?
This is probably the #1 topic veterinary professionals hear about or constantly get trashed for due to requiring deposits or upfront payments before hospitalization or large procedures, not offering payment plans, etc.
Please take into consideration how many clients we see every day that are in situations just like yours. We absolutely understand that life happens, things come up, animals get sick, etc. However, clients need to remember that although it may be a sudden emergency or unique situation for them, it is likely the 4th, 5th, 6th, or 15th similar situation we’ve seen just that day. Other clients before and after will have the same issue — they just paid rent or had car repairs, and don’t have money. Or their cat also just started urinating blood that day, their dog also just ate their underwear that morning, etc. It does NOT trivialize or lessen the experience each of those clients is going through, nor make us less committed to caring and finding solutions, but it does change the overall perspective when you realize that you aren’t the only one.
So when a client asks us to please bend the rules for them, they are joining several others that day that also already asked for free services, surgery without deposits, or a payment plan. How can we possibly do that for all of them? Or how do we pick and choose who we do it for and who we do not? What about all those who never follow through on payment plans and end up getting sent to collections? Unfortunately that is what happens in most cases.
If we took that kind of risk for every single client in that situation, we would end up shuttering our doors. Veterinary medicine is a business, as unfortunate as it is, and like any other business, we cannot lose money or we cannot keep our doors open. If we cannot keep our doors open, we cannot help ANY animals at all. That defeats the entire purpose of what we do and why we exist. In order to counteract all the non-payers, we’d have to greatly increase our prices to compensate — $1000 CT scans instead of $250 — which helps less people, and none of our clients would appreciate that. Why should a paying client have to pay more to cover for someone else’s inability?
Think of it like this:
If you go to the grocery store, fill your basket or your cart, then get to the front and tell the cashier “Sorry, I can’t afford this”…do they let you just walk out the door with your groceries? Or if you did the same at a mechanic, or a clothing store, etc? You are expected to pay for products provided or services rendered. If you cannot afford these things, then you go to a local food pantry, or apply for financial assistance from organizations designed to help those issues. You wouldn’t expect the business to finance you directly or to give you their products/services based on your word that you will pay them back. So why expect it of your veterinary practice? We work with multiple non-profit organizations and outside lenders like Care Credit to offer financial assistance for clients who need it. Many clients often mention that their credit is not worthy of approval by companies like Care Credit. As unfortunate as that is, you have to look at it from our business perspective. If a financial lender does not deem someone credit-worthy to extend a loan to, how should we trust that same person to repay a payment plan?
Our animal hospital here in Chattanooga is one of around 85 practices in the area, which is a ridiculously high number in a metro area of about 400,000 people. Out of those 85, we are one of, if not THE, lowest priced in terms of products, services, surgeries, etc. Our business model is based on low-cost, high-volume, high-quality. Because of this, we are able to help an immense number of owners keep their pets healthy and save them when something unfortunate happens. We are able to offer this kind of pricing and help to our 155,000+ patients without compromising availability, quality of care, quality of supplies and products, knowledge and training, technological availability, and sterility of environment/tools.
How? Because we eliminated the vast majority of risk that goes along with unguaranteed payment plans, services rendered without up front payment, allowing owners to surrender animals into our care, etc. We don’t have to force our great clients to cover for those that take advantage, nor cover the costs for an endless succession of charity cases (which down here in this part of the South would be 3-5 per day).
It’s a very hard position to take, because our hearts would rather take care of EVERYONE regardless of money. That’s why every single one of us went into veterinary medicine, doctor and technician alike. But the realities of our business model and the social area we live in here teach us that we can’t do that, as much as we want to, and a combined 60 years in practice between our two owners has taught them that unfortunately a hard line is necessary if we want to be able to keep taking care of people and pets.
We still have some risk — for example, PJ was a cat who was brought in on death’s door and hospitalized with a treatment plan that the owners elected, only to have them disappear after a week, bail on their entire bill, and leave their cat with us for 2 months. We finally followed the Tennessee state law, gave them one last chance notification via certified letter, and when we got no response, he became our legal property, was treated and surgery was performed, he was then found a loving home, and we ate the $2100 bill. That was a moment where we attempted to work with an owner and it came back to bite us.
Are all clients that way? Absolutely not, and we know that. Several months back, a couple brought in their 1-year-old cat who was HBC (hit-by-car) and had a destroyed femur and pelvis. He needed surgery to fix his injuries or he’d never walk again and would need to be euthanized. They were completely broke, and were despondent in trying to figure out how to make it work. We offered CareCredit and PaymentBanc, neither of which were options for them. They had filed their taxes and were just waiting for their refund to direct deposit, and even had the notification from the IRS saying it would be deposited Wednesday — 2 days from the day we saw them. Finally the doctor (who is one of the two owners) said that if they at least pay the charges from that day, then to go ahead and schedule the cat’s surgery for Wednesday, and if for some reason their refund didn’t deposit, we would figure something out. Sure enough, their money came in, and they brought the cat in for surgery and it was a success. He’s walking and playing normally now. The doctor did what he could to work with the owners and it paid off for both sides.

Peanut, my Soul Cat, who passed away suddenly at just 3 years old.
As pet owners ourselves, we have all been in positions where our animal needed something and the cost was daunting. We weren’t always veterinary professionals, and no, most of us don’t get free services at our own clinics unless we own it. So we absolutely do understand! Unfortunately there is no possible way to differentiate between those clients who will follow through and those who don’t, and unfortunately the latter dominates. PJ’s owners had him for 9 long years and clearly loved him, there was zero doubt when they first brought him in and we went over everything. They just found themselves in a difficult place and didn’t know what else to do, so they disappeared.
Unfortunately all that did is reinforce our policies regarding estimates and requiring payment up front, and prove why we need to stick to it.
In conclusion (finally!)…
Before you get upset when your Vet provides an estimate for a treatment or surgery that costs several hundred to several thousand dollars, please keep in mind everything that goes into that pricing and the area you live in. Even a simple office/exam fee is paying for the availability, education, experience, knowledge, and time of the technician and doctor that see your pet.
Before you get upset that your Vet will not offer a payment plan or perform a surgery/treatment without a deposit or payment up front — please don’t be mad at them, be mad at all the clients who came before you and ruined it for everyone else by forcing that clinic to change policies and become strict.
Before you post an angry emotion-driven Yelp review or viral Facebook post, please consider both sides of the situation, the actual medical case itself vs. the feelings involved, and the impact such an review/post can have on the veterinary hospital or employees involved. It may be the last straw needed to break the camel’s back, and cost someone their life.
The bottom line is that we are here to help animals, and these are the issues and elements that go into being able to do exactly that. Hopefully this aids in a better understanding and improved relationships!
